
Your Parent Is Losing Their Balance. The Wrong Equipment Makes It Worse.
Maybe it started with furniture walking — your mother gripping doorframes and countertops as she crosses the kitchen, pretending nothing has changed. Maybe it was the near-miss on the front steps. Or maybe it's already past that: a hospital discharge planner just told you to "have a walker ready at home by Thursday," and you're staring at 200 options online with no idea which one fits, which one is safe, and which one Medicare will actually cover.
Here's the part no one warns you about: a poorly chosen mobility aid doesn't just fail to help — it actively increases fall risk. A rollator that rolls too easily under a parent with poor bilateral balance. A walker sized too high, forcing a hunched forward lean that destroys what stability remains. A cane used on the wrong side, pulling body weight in the wrong direction. One in four adults over 65 falls every year, and in too many cases the equipment itself is the problem.
The information you need exists — buried across Medicare PDFs, physical therapy blogs, FDA safety bulletins, and senior-care portals funded by the assisted living facilities they're quietly steering you toward. What doesn't exist anywhere is the complete sequence: assess the actual problem, measure your parent, choose the right device for their specific limitation, get insurance to cover it, make the home safe, and handle the conversation when they refuse to use it.
The Clinical Sizing and Funding Blueprint
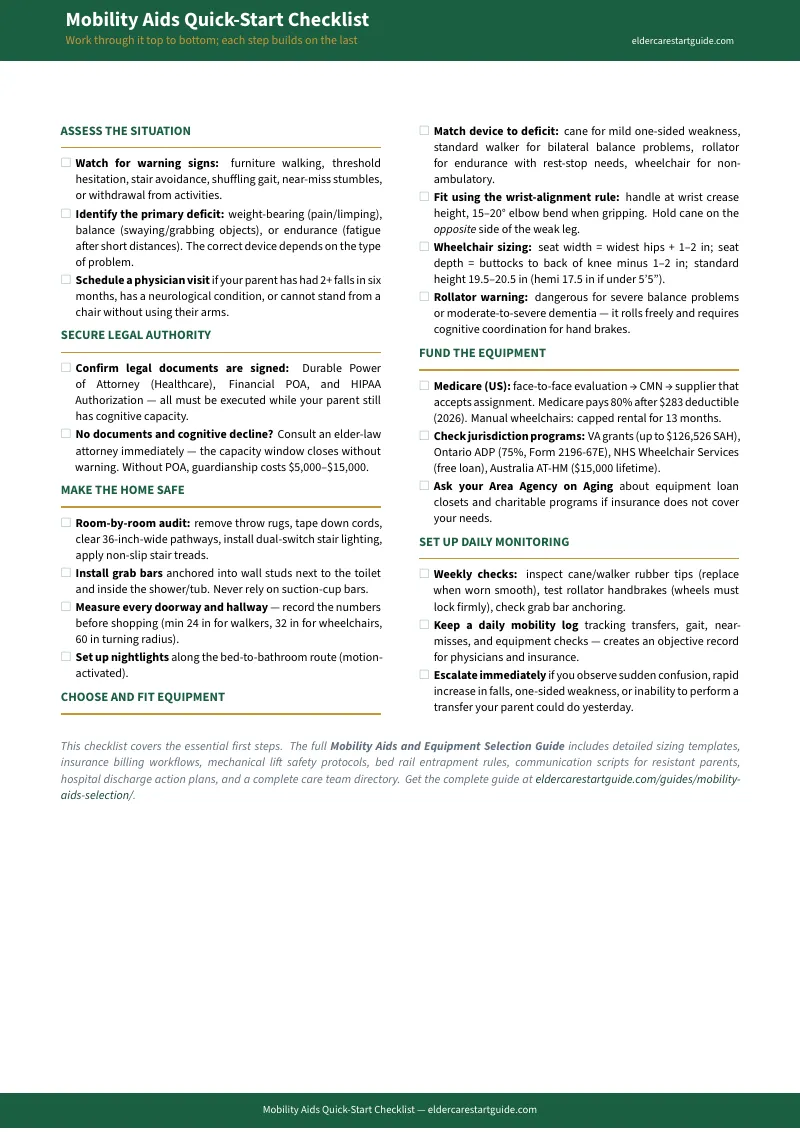
The Mobility Aids and Equipment Selection Guide isn't a product catalog or a brand comparison. It's a clinical-grade sizing, funding, and implementation system — the exact measurement steps, comparison frameworks, insurance billing sequences, and home safety audits that a physical therapist and an elder law attorney would walk you through, compressed into a single toolkit you can use tonight.
Where free resources give you general advice to read, this guide gives you measurement templates to fill in, comparison tables to decide with, and billing checklists to submit. Every page has a specific job: size a device, assess a room, prepare for an insurance claim, script a difficult conversation. Complete one worksheet and you've made measurable progress — even if you only have fifteen minutes between work calls.
What's Inside
- Three-Category Functional Assessment — because "they need a walker" isn't a diagnosis. This clinical framework helps you identify whether your parent's primary limitation is weight-bearing (orthopedic pain), balance (neurological/sensory), or endurance (cardiovascular/pulmonary) — and maps each category directly to the correct device type. The right device depends on the type of problem, not just the severity.
- Device-by-Device Comparison Tables — canes, standard walkers, rollators, transport wheelchairs, and manual wheelchairs compared side-by-side on weight-bearing capacity, stability, cognitive demand, and clinical indicators. A cane supports up to 25% of body weight; a standard walker supports up to 50%. A rollator requires good grip strength and balance to manage hand brakes — making it actively dangerous for a parent who leans heavily on their device. These tables eliminate the guesswork.
- Clinical Sizing Measurements — the exact measuring steps professionals use. Walker sizing: the wrist-alignment rule (handle grip aligns with the crease of the wrist when standing upright with relaxed arms). Wheelchair sizing: seat width (widest hip point plus 1–2 inches), seat depth (buttock to knee minus 1–2.5 inches), seat-to-floor height (hemi-height at 17.5 inches for users under 5'5", standard 19.5–20.5 inches). Printable templates you can fill in at home.
- Medicare Part B Reimbursement Blueprint — the step-by-step billing sequence that gets equipment covered. The face-to-face physician exam requirement, the written order specifying in-home medical necessity, the enrolled-supplier and accept-assignment rules, the 80/20 coinsurance split after the Part B deductible, and the capped-rental pathway where ownership transfers after 13 months. Plus Medicaid HCBS waiver coverage, VA benefits, and community equipment loan closets.
- Room-by-Room Home Safety Audit — a printable walkthrough for every room in the house. Doorway width clearances (32 inches minimum for wheelchairs, 36 for walkers), threshold ramp specifications, cord management, furniture layout for turning radius, lighting upgrades, and the bathroom — the most dangerous room. Grab bar anchoring rules (never into drywall alone), transfer bench setup, and non-slip specifications.
- Specialized Equipment Safety Guide — lift chairs (2-position vs. 3-position vs. infinite-position, Medicare coverage of the motor mechanism only), bed rails (the FDA's critical under-4.5-inch gap rule to prevent entrapment — and why bed rails must never be used as restraints for a parent with dementia), stair lifts, transfer aids (gait belts, transfer boards, Hoyer lifts), and the clinical threshold where manual lifting must stop entirely.
- 48-Hour Hospital Discharge Action Plan — because when your parent is being sent home tomorrow, you need a crisis-mode checklist, not a research project. Rent-vs-buy decisions for short-term recovery equipment, the critical four-step discharge setup (walker-accessible entryway, hospital bed rental, raised toilet seat, home-health transition), and how to get DME ordered and insurance-approved before your parent leaves the facility.
- Resistant Parent Conversation Scripts — word-for-word scripts for the conversation that stops most families cold. Why resistance is fear of losing control, not stubbornness. The "accessory with benefits" reframing that works. How to use a doctor-ordered PT evaluation so the recommendation comes from a trusted professional rather than an anxious adult child.
- Daily Monitoring and Care Team Framework — how to spot the signs that the current device is no longer enough and it's time to step up. Gait monitoring, proper accompaniment technique (beside or behind, never in front), maintenance schedules, and the care team roster — PT/OT, primary care, DME supplier, elder law attorney — so no single person carries it alone.
- Legal Readiness Checklist — the paperwork that must happen before cognitive decline closes the window. Durable Power of Attorney, Healthcare Proxy, what to sign and in what order, and how organizing your files first lets you use an elder-law attorney with surgical efficiency instead of paying them $195–$500 per hour to sort your paperwork.
Who This Is For
- Adult children who just noticed the furniture walking — or just got the call about a fall — and need to know what to do before the next one happens
- Families facing a hospital discharge deadline and told to "have a walker ready" with no guidance on which one, what size, or how to pay
- Caregivers trying to get Medicare or insurance to cover equipment they've been told costs hundreds out of pocket
- Long-distance sons and daughters who can't be there to measure doorways and test the shower chair in person
- Spouses managing their own physical decline who need to minimize their own injury risk during transfers and daily care
- Families stuck in the resistance loop — a parent who needs a mobility aid but refuses to use one
Why Free Resources Aren't Solving This
Medicare.gov explains the rules. AARP publishes the articles. WebMD lists the device types. But none of them give you the step-by-step implementation sequence — the system that takes you from "my parent is unsteady" all the way through "the right device is fitted, funded, installed, and being used safely."
Large senior placement platforms like A Place for Mom and Caring.com are funded by commissions from the facilities they recommend. Their content naturally steers you toward institutional placement rather than helping you keep your parent at home safely. Government sites provide dense regulatory language designed for compliance officers, not for a stressed adult child reading on their phone at midnight.
This guide carries zero commercial bias. We don't sell walkers, and we don't accept commissions from care homes or equipment manufacturers. What you're getting is a clean, conflict-free implementation sequence — saving you dozens of hours of fragmented research and protecting you from the high-pressure sales funnels that dominate the elder care space.
The Pre-Consultation Blueprint
A physical therapy home evaluation runs $150–$300 out of pocket. A geriatric care manager charges $100–$250 per hour. An elder-law attorney charges $195–$500 per hour. Every minute they spend collecting your parent's home measurements, medical history, or legal documents is money you could have saved by arriving prepared.
This guide is your preparation layer. When you show up to the PT evaluation with a completed functional assessment, accurate home measurements, and a fitted equipment profile — the professional starts working on your parent's problem instead of gathering your data. One organized consultation can replace three disorganized ones.
100% Satisfaction Guarantee
If this guide doesn't help you choose, fund, and implement the right mobility solution within 30 days, email us for a full refund. No questionnaires, no hassle. You're navigating one of the hardest transitions of your life — the last thing you need is purchase anxiety on top of it.
— Less Than One Professional Visit
One PT home evaluation costs $150–$300. One hour with a geriatric care manager runs $100–$250. This toolkit is a fraction of a single professional visit — and it helps you make every professional interaction faster, cheaper, and more productive from the first appointment.
Get the free Quick-Start Checklist to see the system in action, or get the full Mobility Aids and Equipment Selection Guide and start making your parent's home safer tonight.