You're the One Making All the Calls, Running Every Appointment, and Briefing Every Aide — and Nobody Told You There's a Way to Stop Doing This Alone
It started with a few extra errands. Picking up prescriptions. Driving to one more specialist. Calling to reschedule the aide who didn't show. Then the hospital discharge happened, and suddenly you were managing three rotating caregivers, coordinating with a cardiologist and a neurologist and a physical therapist, fielding texts from siblings who wanted updates but never took a shift, and keeping your parent's insurance paperwork from burying you alive — all while holding down your own job and family.
You're not lazy. You're not disorganized. You're doing the work of a care coordinator, a nurse liaison, a shift manager, and a family mediator — with no training, no backup plan, and no system. And the longer you run everything from memory and sticky notes, the higher the stakes get: a medication change that didn't reach the Tuesday aide, a legal document nobody can find at 2 a.m., a sibling who insists Mom is "doing fine" because they haven't seen the daily reality.
The free checklists on AARP and Caring.com tell you to "create a care plan." They never hand you the actual tools to build and run one.
The Care Team Coordination System
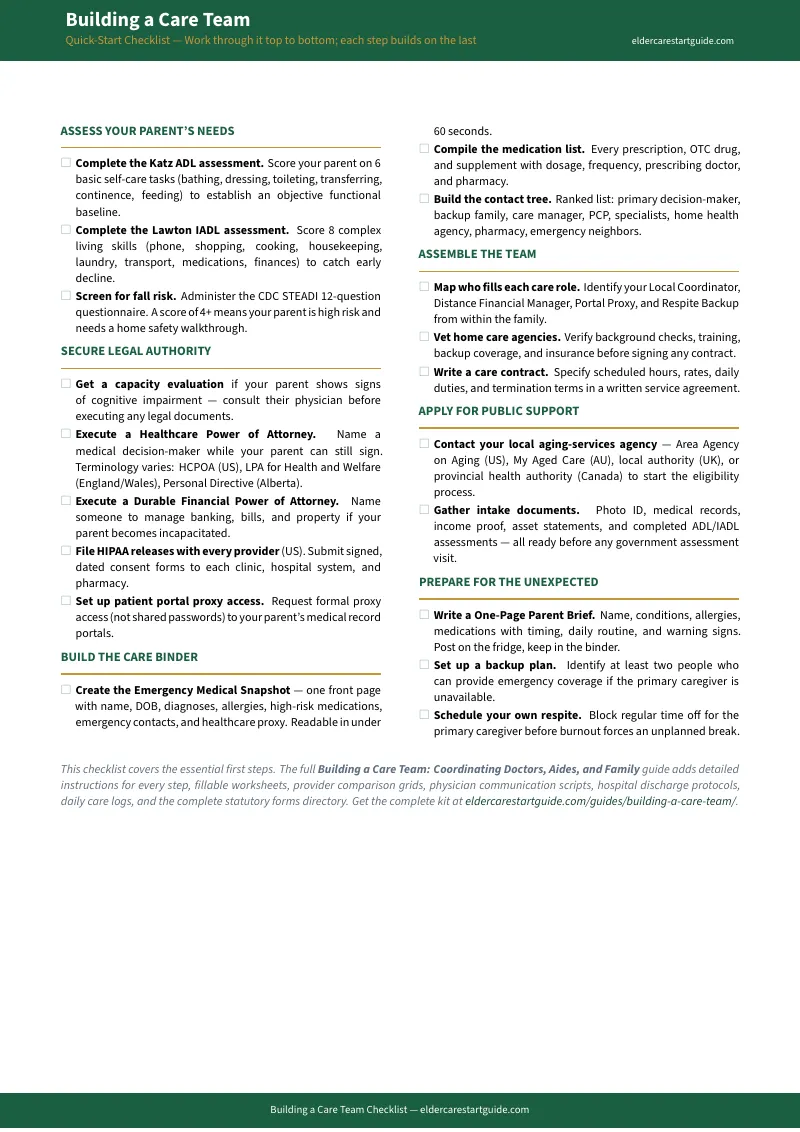
This guide is built around one structural problem that free resources never solve: the information lives in your head, and it needs to live in a system anyone on the team can access. Instead of scattered notes and secondhand phone updates, you get one connected framework that moves you from solo caregiver to team coordinator — with defined roles, shared logs, standardized handoffs, and a backup plan for the day you can't be there.
At its core is the Functional Baseline Assessment: a structured way to document exactly where your parent stands right now — mobility, cognition, medications, daily routines — so every conversation with a doctor, aide, or sibling starts from shared facts instead of subjective impressions. When your brother in Denver says "Dad seems fine on the phone," you have the daily log that shows he needed help with bathing three times this week and forgot his afternoon medication twice.
What's Inside
- The Care Team Role Directory — a structured role-assignment system based on proximity, capacity, and skills, not guilt or obligation. Specific assignments for the local coordinator, the long-distance financial manager, the medical liaison, the legal point person, and the backup respite coordinator. Every person knows exactly what they own and what they don't.
- The Care Binder Architecture — the exact tab structure, document list, and emergency-access protocol for a physical binder that any family member, aide, or EMT can navigate in under sixty seconds. Medical contacts, medication lists, legal documents, insurance cards, daily routines, and emergency instructions — organized so the information finds the person who needs it, even in a crisis.
- The Daily Care Log & Shift Handoff System — standardized logs for tracking medication administration, meals, mobility, mood, bowel function, and behavioral changes across multiple caregivers and shifts. When Tuesday's aide leaves and Thursday's aide arrives, nothing falls through the crack. When the doctor asks "how has she been this week?" you hand over data, not guesses.
- The Family Care Meeting Kit — a ready-to-run meeting agenda with ground rules, decision frameworks, and commitment-tracking templates. Covers clinical status review, financial spend updates, legal authority checks, and task redistribution. Includes guidance on neutral facilitation for families where conversation regularly turns into argument.
- The Provider Communication Templates — doctor visit preparation sheets (the three questions to bring, the medication list format doctors actually want, the follow-up documentation protocol), specialist referral trackers, and pharmacy coordination checklists. Stop leaving appointments thinking "I forgot to ask about the new tremor."
- The Private Provider Vetting & Hiring Guide — interview questions, reference-check scripts, and trial-period evaluation criteria for home health aides, companion caregivers, and geriatric care managers. Background check requirements, contract red flags, and the specific questions that separate experienced aides from undertrained ones.
- The Public Program Navigation Maps — jurisdiction-specific pathways for US (Area Agencies on Aging, Medicaid HCBS waivers, VA Aid & Attendance), Canada (provincial home care authorities), Australia (My Aged Care, ACAT assessments, Home Care Packages), and UK (local authority needs assessments, NHS Continuing Healthcare). Know exactly where to apply and what to ask for.
- The Hospital Discharge Coordination Plan — the 72-hour post-discharge protocol covering medication reconciliation, DME delivery, home safety modifications, follow-up scheduling, and the specific questions to ask the discharge planner before you sign anything. Built around the clinical IDEAL framework so nothing critical gets missed in the pressure of "we need the bed."
- The Emergency Backup Protocol — a "springing" plan that activates automatically when the primary caregiver is sick, traveling, or unavailable. Pre-identified backup contacts, a one-page parent brief for temporary aides, and an escalation ladder from "aide called in sick" all the way to "primary coordinator is in the hospital herself."
- The Professional Escalation Guide — when to bring in a geriatric care manager ($100–$250/hr), an elder law attorney ($200–$500/hr), or a Medicaid planner — and how to walk into that first meeting fully organized so you're paying for strategic advice, not basic discovery. One organized consultation can replace five disorganized ones.
Who This Is For
- The adult child who became the default care coordinator and is managing everything from their own kitchen table — aides, doctors, medications, finances, family drama — without a system or a backup
- Long-distance family members who want to contribute meaningfully but can't be physically present, and need a clear role and a shared information framework
- Families where sibling conflict over caregiving is driven by unequal workloads, different perceptions of the parent's condition, or a complete absence of shared documentation
- Anyone managing rotating home health aides and losing critical information between shifts — medication changes, behavioral observations, task completions
- The crisis-driven sibling thrown into coordination overnight after a fall, stroke, or hospital admission — who needs a functional system by the end of the week, not a philosophy of care
Why the Free Resources Leave You Stuck
AARP publishes excellent caregiving overviews. The NHS has anticipatory care templates. Area Agencies on Aging offer fragmented PDF forms. None of them hand you a fillable daily care log, a shift-handoff template, a family meeting agenda with ground rules, or an emergency backup protocol you can activate tonight. They describe what care coordination is. This guide is the operating system that makes it work.
Then there are the referral portals — A Place for Mom, Caring.com — whose business model runs on commissions from assisted living facilities. Their content is structurally designed to convince you that in-home care coordination is too complex to manage yourself. Hand over your phone number and the sales calls start. This guide takes the opposite position: your family can run a coordinated care team at home, and the system to do it costs less than one hour of a geriatric care manager's time.
Satisfaction Guarantee
If this guide doesn't give you at least one coordination tool, communication template, or organizational framework you weren't using before, email us for a full refund. No forms, no waiting period. The only risk is continuing to carry everything yourself.
Stop Being the Only One Who Knows Everything
Download the free Quick-Start Checklist for the one-page care team coordination overview — or get the complete Building a Care Team: Coordinating Doctors, Aides and Family for and have every log, template, meeting agenda, and backup protocol you need to build a care team that actually functions — even when you're not in the room.